
Among 7 Positive Emotions, Awe Had the Strongest Link to Lower Inflammation
There’s a general understanding that positive emotions are good for your health, and negative emotions are bad for it. While true, it’s slightly vague; it’s a bit like saying “exercise is good for you” without distinguishing between a walk around the block and a deadlift.
A study from UC Berkeley, led by Jennifer Stellar and colleagues and published in the journal Emotion, tried to get more specific. The researchers looked at seven distinct positive emotions and asked whether they related differently to a biological marker of inflammation. The answer was yes.
And the emotion with the strongest association wasn’t joy, or love, or even gratitude. It was awe.
What the Study Measured
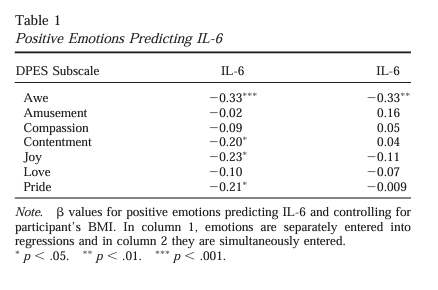
The researchers studied 218 healthy young adults across two samples (119 in one, 99 in a second). Each participant reported how frequently they experienced seven positive emotions: amusement, awe, compassion, contentment, joy, love, and pride. Then the researchers collected oral mucosal samples and measured levels of interleukin-6 (IL-6), a proinflammatory cytokine that’s involved in the body’s inflammatory response.
IL-6 isn’t a measure of “immune strength.” It’s a measure of inflammatory activity. When IL-6 is elevated over time, it’s generally a sign that the body is in a chronic inflammatory state, which is associated with everything from cardiovascular disease to depression to chronic pain.
So the study wasn’t asking “do positive emotions boost your immune system?” It was asking something more precise: among several positive emotions, which ones are most closely associated with lower inflammation?
The Results
At the broad level, people who reported more positive emotions overall had lower IL-6. That’s consistent with existing research. The more interesting finding was what happened when they broke the emotions apart.
Awe showed the strongest and most consistent association with lower IL-6 across both samples. Compassion and contentment showed some association in certain analyses, but awe was the one that held up most reliably. The other emotions — amusement, joy, love, pride — didn’t show the same pattern.
To be clear about what this means and what it doesn’t: this was an observational study. People who reported experiencing more awe also tended to have lower inflammation.
The study can’t tell us that awe directly caused the lower IL-6. It shows an association, not a mechanism. That’s an important distinction, and the authors were careful about it.
Why Awe Might Be Different From Other Positive Emotions
So why awe, specifically? The study didn’t test a mechanism, but the researchers offered a hypothesis that’s worth considering.
Awe tends to be triggered by experiences that feel vast or larger than your usual frame of reference. Standing at the edge of a canyon. Listening to a piece of music that stops you mid-thought. Watching something unfold that you can’t quite fit into your existing understanding of how things work. The common thread is that awe shifts your attention outward — it pulls you out of self-focused processing.
That’s different from, say, amusement (which is usually reactive) or pride (which is self-referential). The researchers suggested that awe’s tendency to reduce self-focus may be part of why it relates differently to inflammatory biology.
When you’re in a state of awe, you’re not ruminating. You’re not threat-monitoring. You’re not running the mental loops that tend to keep the stress-inflammation axis activated.
That’s a hypothesis, not a proven mechanism. But it’s a reasonable one, and it connects to things we understand about how the nervous system regulates inflammation.
Why This Matters for Chronic Pain and Neuroinflammation
Chronic Pain Is an Inflammatory State
IL-6 is one of the proinflammatory cytokines that’s elevated in many chronic pain conditions — fibromyalgia, central sensitization syndromes, persistent musculoskeletal pain.
Chronic elevation of IL-6 feeds neuroinflammation, which amplifies pain signaling, disrupts mood, and contributes to the kind of brain fog and emotional fatigue that chronic pain patients know well.
Anything that’s reliably associated with lower IL-6 is worth paying attention to; it’s a data point about what kinds of experiences might support a less inflamed internal environment.
The Self-Focus Connection
One of the hallmarks of chronic pain is what researchers call hypervigilance: the brain’s constant monitoring of bodily sensations, scanning for threat, evaluating and re-evaluating whether something is dangerous. It’s exhausting, and it’s self-focused by nature. Pain keeps your attention locked inward.
If awe’s anti-inflammatory association has something to do with shifting attention outward and interrupting self-focused processing, that’s interesting in the context of treatments we already use.
Pain Reprocessing Therapy (PRT) works in part by helping patients reappraise pain signals and break the hypervigilant monitoring cycle. Ketamine-assisted psychotherapy often produces experiences that patients describe in terms that sound a lot like awe — a sense of expanded perspective, connection to something larger, a temporary loosening of rigid self-referential thought patterns.
None of that means awe is a medical treatment. But it suggests that the experiences and emotional states that accompany effective therapy may not be incidental. They may be part of why the therapy works.
The Lifestyle Layer
There’s also a practical dimension here that doesn’t require a prescription. Experiences that tend to produce awe — time in nature (a remarkable sunset or sunrise…that feeling when you stand at the water on the beach and realize you are so small compared to the entire ocean lapping at your feet), exposure to art or music, moments of genuine wonder — are the kinds of things that often fall away when someone is managing chronic pain. The world gets smaller. Routines get rigid. The range of experience narrows to what feels safe.
This study doesn’t prove that going to a national park will lower your IL-6. But it’s consistent with a broader body of research suggesting that expanding your range of emotional experience, especially in directions that pull attention outward, may have real physiological relevance.
For patients in our practice, we often talk about this as part of the environment (and method) that supports healing.
What This Study Doesn’t Tell Us
A few things worth keeping in perspective:
The participants were healthy young adults. We don’t know if the same pattern holds in older populations, in people with chronic illness, or in different demographic groups.
It was observational. The association between awe and lower IL-6 could be influenced by other factors the study didn’t measure. People who experience more awe might also be more physically active, or have lower baseline stress, or differ in other ways.
The study measured a single cytokine. IL-6 is a useful marker, but the inflammatory system is complex. A full picture would involve multiple markers and longitudinal data.
Awe is not a treatment. It’s an emotional experience that showed an interesting statistical association. That’s a meaningful research finding, not a prescription.
The value of this study is that it adds specificity to the relationship between emotional experience and inflammatory biology. Not all positive emotions are the same, physiologically. That’s useful to know.
The Bottom Line
The broad advice to “think positive” has never been particularly helpful for people dealing with real health problems. It often feels to broad and fluffy to implement anything actionable.
This study is interesting because it moves past that and asks a better question: are there specific emotional experiences that relate to inflammation differently?
The answer, at least in this sample, is yes. Awe — the experience of encountering something vast, something that momentarily pulls you beyond your own frame of reference — showed the strongest link to lower IL-6 among the seven emotions studied.
For anyone managing chronic pain or neuroinflammation, that’s not a treatment plan, but it is a little less fluffy to have a direct instruction to make an effort to make an effort to stand under the trees, catch a sunset, look at the ocean horizon, or listen to music that gives you chills.
Learn More
If you’re interested in how we integrate the science of inflammation, neuroplasticity, and emotional experience into pain treatment, schedule a consultation with Dr. Weiner’s team at NeuroPain Health.
Read more about our approach to Pain Reprocessing Therapy, Ketamine-Assisted Psychotherapy, and the kynurenine pathway and neuroinflammation.
Reference
Stellar JE, John-Henderson N, Anderson CL, Gordon AM, McNeil GD, Keltner D. “Positive affect and markers of inflammation: Discrete positive emotions predict lower levels of inflammatory cytokines.” Emotion. 2015;15(2):129–133. PubMed | Full text (PDF)